Myopia
What is myopia?
Nearsightedness, or myopia, as it is medically termed, is a vision condition in which people can see close objects clearly, but objects farther away appear blurred. Myopia occurs if the eyeball is too long or the cornea (the clear front cover of the eye) is too curved. As a result, the light entering the eye isn't focused correctly, and distant objects look blurred. Myopia affects nearly 30% of the U.S. population.

What causes myopia?
Both genetic and environmental factors are believed to play a role in the development of myopia.
Children with a parent who is myopic are more likely to be myopic themselves.
Additionally, children who spend considerable time reading, working at a computer, playing video games or doing other intense close visual work may be more likely to develop myopia.
Other factors that play a role in developing myopia are not yet fully understood. In special cases, myopia may be related to other medical or eye problems, but here we are discussing the more common form of near-sightedness.

Myopia is influenced by genetic and environmental factors
Dr. Topete is the only member of her family who is myopic and starting using glasses when she was a child. She spent many hours using her vision at near (reading, studying and playing hand held video games). Her myopia is primarily environmental.
Dr. Topete’s daughter has a higher risk of becoming myopic too because both her parents are myopic.
What are symptoms of myopia?
People with myopia can have difficulty clearly seeing a movie or TV screen, a whiteboard in school or while driving. They may also experience eye strain, headaches and often squint. Generally, myopia first occurs in school-age children. Because the eye continues to grow during childhood, it typically progresses until about age 20. However, myopia may also develop in adults due to visual stress or health conditions such as diabetes.
Will my child’s myopia increase forever?
Nearsightedness is often discovered in children when they are between ages 8 and 12 years old. During the teenage years, when the body grows rapidly, myopia may become worse. Between the ages of 20 and 40, there is usually little change.
How can you know if a child has myopia if they can’t talk or read letters yet?
In a patient too young to read the letters on an eye chart, your optometrist/ophthalmologist can use a device called a retinoscope to measure where light is being aimed inside the eye. This allows an ophthalmologist/optometrist to measure a young child’s glasses prescription. This is often used after dilation drops to obtain the most accurate results.
Myth: “I don't want my child to wear glasses because then they will become dependent on them and it will make their vision worse”
Myopia continues to progress in most affected children whether or not they wear glasses. Not wearing eyeglasses, or wearing an incorrect prescription, can cause your child to experience blurriness, eye strain and other uncomfortable symptoms. If these issues aren’t addressed, they can impact your child’s quality of life dramatically and make school much harder than it needs to be.
It should be noted that vision continues to develop throughout childhood, so your child’s vision may not be the same now as it was one year ago. It’s normal for a person’s vision to change as the eyeballs grow and the visual system develops. In fact, your eyesight doesn’t begin to “level out” until you reach your 20s.
So if it seems like your child’s vision is getting worse as they get older, it could simply be that it’s part of the natural development of their eyesight — not from going without glasses.
A few general recommendations:
Monitor working distance - typically it is recommended that near working distance be no less than the distance between your knuckles and your elbow.
Take breaks - use the 20/20 rule. A twenty second break is recommended after every 20 minutes of near work, even if only for a few moments of distance viewing.
Go outside and play – recent studies have shown that children who spend time outdoors each day were less likely to be nearsighted and had lower levels of nearsightedness than their peers who spent less time outdoors.
What can be done to prevent worsening of myopia once it has been detected?
Although myopia can progress at very different rates in different children, once children become nearsighted, their prescription is expected to progress by 0.50D per year, on average. Many researchers are investigating ways to slow, or even stop the worsening of myopia. When considering whether to request any of these methods, please keep in mind that not all children with myopia respond to any given treatment, and the long-term effectiveness of many of these treatments has not been proven. Additionally, long-term treatment may be needed to prevent relapse.
A great first step to prevent or slow the progression of nearsightedness is to encourage your child to spend more time outdoors. Balancing indoor time with outdoor time is beneficial for a child’s health and well-being. Outdoor time is protective against nearsightedness and a good prescription for eye health.
Low dose atropine (eye-drop medicine). Daily use of low-dose atropine eye drops slows the progression of nearsightedness in children and teenagers. The drops are placed in each eye at bedtime. These drops keep the eye from lengthening too much, because nearsightedness worsens as the eye grows longer. Patients must use the drops once a day for several years. These drops stop or slow the progression of nearsightedness in 80 percent (8 out of 10) of children. Side effects of atropine drops at low doses may include light sensitivity, redness or itchiness around the eye. There are different concentrations of atropine available and your doctor may adjust the dosage to balance out side effects and treatment outcomes.
Orthokeratology (ortho-k). Orthokeratology uses hard contact lenses to temporarily flatten the cornea and reduce nearsightedness. Patients must sleep in hard contact lenses every night. There is a risk of serious, vision-threatening eye infections with orthokeratology, especially if they are not cleaned/used properly (the same risk as all contact lenses).
Multifocal contact lenses/ Peripheral defocus contact lenses are special contacts. They are made for children 6 to 12 years of age with nearsightedness. These lenses have different areas of focus. This type of lens looks like a dartboard, with multiple circles inside of each other. The center of the lens corrects blurry distance vision, while the outer parts of the lens blur the child’s peripheral (side) vision. Blurring side vision is thought to slow eye growth and limit nearsightedness.Like any contact lens, there is a risk of getting a corneal infection. Be sure your child can correctly wear, clean, and store the contact lenses to avoid infection.
There is no scientific evidence to suggest that eye exercises, vitamins or pills can prevent or cure myopia.
Myopia control options to consider and discussed with your doctor:
Atropine
Pros:
Currently the most effective in myopia control option (on average slows progression about 77%)
Mailed directly to your address.
Cons:
Side effects of the drops (depending on the strength) may include dilated pupil and blurry vision at near.
Your child will still need to use glasses
Not be recommended in children with heart conditions.
Pharmacy: Imprimis Rx
Cost: $117 for a 3 month supply
Phone to call: 844-446-6979
Text: 858-462-2082
Low dose atropine is offered at Children’s Hospital Los Angeles. If interested to see if your child would be a good candidate for contact lenses, schedule an appointment with your local optometrist.

Low-Concentration Atropine for Myopia Progression (LAMP) Study- A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control
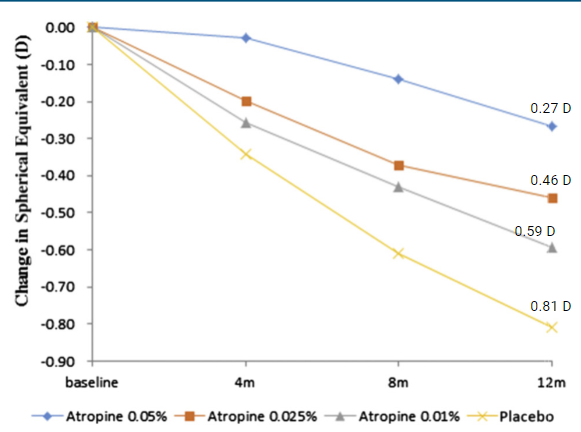
Concentration-dependent response on myopia control was observed in all atropine concentrations. From the LAMP study (phase 1)
Ortho-keratology
Pros:
No need to wear glasses during the day.
Progression slowed by about 30-50%
Cons:
Risk of corneal infection from sleeping in contact lenses.
Most expensive option, often $1000-2000 for fitting and lenses
Must be ideal candidate depending the prescription and shape of the front of the eye

Multifocal contact lenses
Pro:
No need to wear glasses during the day.
Progression slowed by about 30-50%
Cons:
Risk of corneal infection from contact lenses.
More expensive than traditional contact lenses and may be associated with slight blurred vision.
Cost is variable, but approximately $200-300 per year.
Least effective in reducing progression of myopia.

References/Resources:
Dolgin E. The myopia boom. Nature 2015;519(7543):276-8.
Mutti, D.O., et al. Parental myopia, near work, school achievement, and children’s refractive error. Invest Ophthalmol Vis Sci, 2002; 43, 3633-40.
He M, et al. Effect of Time Spent Outdoors at School on the Development of Myopia Among Children in China: A Randomized Clinical Trial. JAMA. 2015;314(11):1142-48.
Goss DA, Cox VD. Trends in the change of clinical refractive error in myopes. J Am Optom Assoc. 1985; 56:608-13
Leo SW. Current approaches to myopia control. Curr Opin Ophthalmol 2017;Publish Ahead of Print.
Smith MJ, Walline JJ. Controlling myopia progression in children and adolescents. Adolesc Health Med Ther 2015;6:133–40.
Mananian, Turpin, Kestenbaum. Myopic contro”Myopia Control: Everything You Need to Know”. Eyes on Eyecare. Dec 2021
Walline, JJ; Walker, MK; Mutti, DO; Jones-Jordan, LA; Sinnott, LT; Gaume Giannoni, A; Bickle, KM; Schulle, KL; Nixon, A; Pierce, GE; Berntsen, DA “Effect of high add power, medium add power, or single vision contact lenses on myopia progression in children: the BLINK randomized clinical trial,” published August 11, 2020 in JAMA. DOI: 10.1001/jama.2020.10834